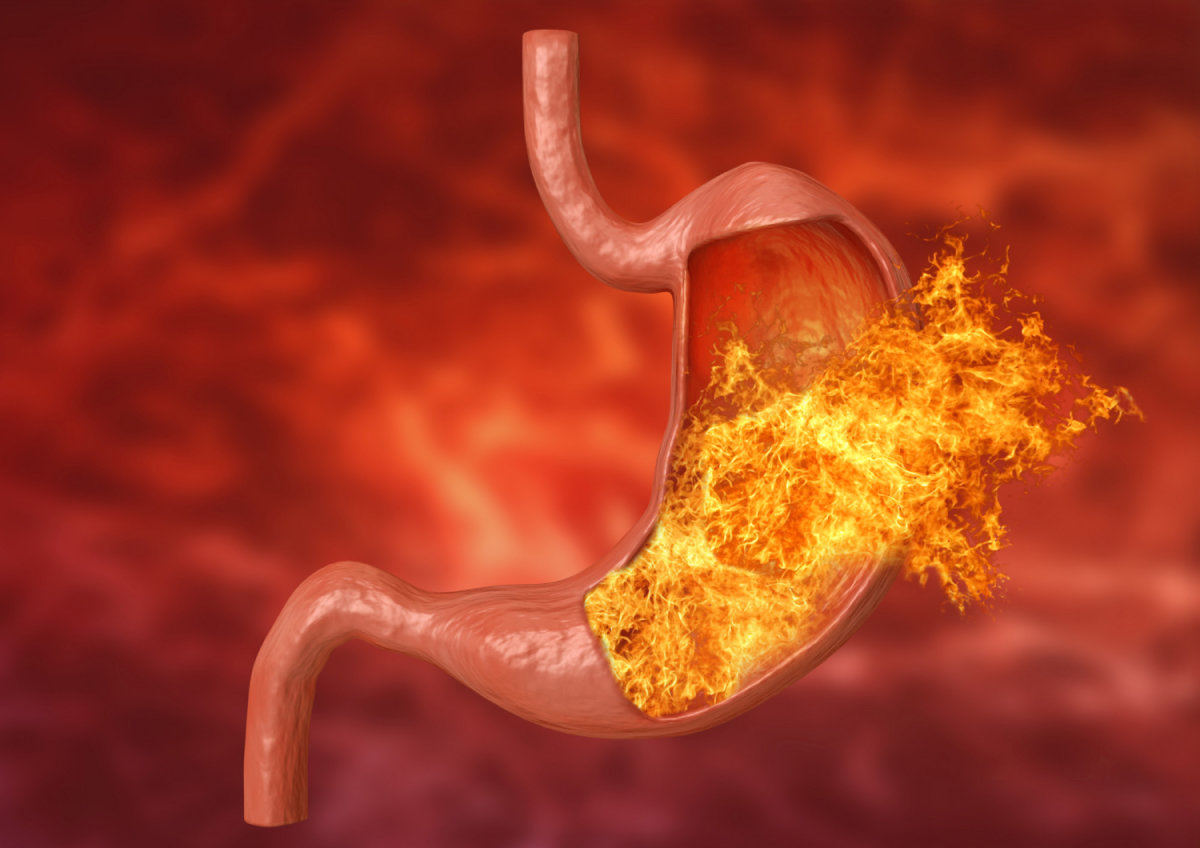
You’re not alone if you deal with acid reflux. This condition affects many people. GERD is a chronic acid reflux condition that keeps becoming more common.
Here’s the good news!
If you’re dealing with those uncomfortable burning sensations, you can usuallytreat GERD by combining lifestyle changes with medication. Simple changes in your daily routine can make a real difference. Your acid reflux diet plays an important role along with other daily habits you can modify. Weight loss helps decrease esophageal acid exposure.
Common Foods That Trigger Acid Reflux
Your diet is a huge part of managing acid reflux symptoms. The foods you avoid are the foundations of a diet that works against acid reflux. Let’s look at the foods that cause those uncomfortable flare-ups.
Fried and fatty foods
Fatty foods rank among the worst triggers for acid reflux symptoms. These foods work against you in two major ways. They keep food in your stomach longer by delaying emptying, which increases acid backflow chances. They also make the lower esophageal sphincter (LES) relax. This valve normally stops stomach contents from flowing backward. Rich, fatty meals, especially fried items like onion rings, french fries, and fatty meats, trigger cholecystokinin (CCK) release. This hormone makes the LES relax.
Citrus fruits and tomato-based products
Citrus fruits like oranges, grapefruits, lemons, and limes can irritate your already sensitive esophageal lining with their high acidity. These fruits and their juices can also reduce LES pressure creating ideal conditions for acid reflux. Tomatoes and tomato-based foods like marinara sauce, ketchup, and salsa cause similar issues. Their acid content relaxes the LES and lets stomach contents flow backward.
Chocolate, peppermint, and caffeine
Chocolate may be delicious, but it contains caffeine, fat, and cocoa, which are all troublesome for acid reflux. Research shows chocolate lowers mean basal LES pressure. Most people think peppermint soothes digestion, but it does the opposite with acid reflux. It relaxes both the LES and other GI tract muscles. Doctors often tell GERD patients to avoid menthol/peppermint oil because it can trigger symptoms. The caffeine in coffee, tea, and some sodas relaxes the LES and boosts stomach acid production. Doses above 200 mg can make the LES relax and cause acid reflux. Research results vary, but some studies link caffeinated drinks to more reflux symptoms while others show no direct connection.
Carbonated drinks and alcohol
The bubbles in carbonated drinks increase stomach pressure and push contents up against the LES. While research isn’t definitive, higher acidity and effects on LES pressure suggest fizzy drinks may make symptoms worse for many people. Alcohol needs special attention because it harms the esophagus in multiple ways. It relaxes the LES and increases acid production.
Foods That Help Reduce Acid Reflux Symptoms
Getting relief from acid reflux goes beyond avoiding trigger foods. Adding specific beneficial foods to your diet can make a big difference in managing symptoms.
High-fiber options like oatmeal and root vegetables
Fiber-rich foods are important for a diet that works against acid reflux. A study shows that adding just 12.5 grams of soluble fiber daily reduced weekly heartburn episodes. Oatmeal stands out as an excellent choice because it absorbs stomach acid and helps regulate digestion. This whole grain keeps you feeling full and prevents overeating.\
Root vegetables play a big role in your acid reflux support plan. Sweet potatoes, carrots, and beets contain soluble fiber that’s easy on digestion. These nutrient-dense vegetables fill you up without being acidic. More importantly, they pack complex carbohydrates that digest slower than simple carbs, which helps control hunger better.
Alkaline foods
The pH scale shows acidity levels, and alkaline foods help counter strong stomach acid. Bananas rank among the best alkaline fruits to fight reflux. Their pectin content helps keep proper digestive flow. These fruits coat irritated esophageal linings and bring quick relief. Melons shine as highly alkaline fruits that neutralize stomach acid. In fact, these fruits link to lower GERD risk.
Watery foods like cucumber and lettuce
Foods high in water naturally dilute and weaken stomach acid. Cucumber packs plenty of water, making it perfect when you want something crunchy without risking a flare-up. Celery works the same way, helping keep irritating stomach acid in check through its high water content. Lettuce gives you the same benefits as other water-rich vegetables. Its high water content helps weaken stomach acid, which reduces reflux-related irritation. Green vegetables like broccoli, asparagus, and leafy greens protect you more through their alkaline properties and low fat content.
Eating Habits That Make a Difference
Your acid reflux management goes well beyond what’s on your plate. How you eat makes a huge difference. Simple changes to your dining habits can improve your symptoms.
Avoiding large meals
You can manage reflux better with smaller, frequent meals. Studies show eating larger portions (600ml vs 300ml) leads to more reflux episodes (17 vs 10) and increases total acid reflux time (12.5% vs 5.5%). Your stomach’s fundus stretches with large meals and puts pressure on the lower esophageal sphincter that stops backflow. The better approach is to “graze” with mini-meals throughout your day to keep digestion steady.
Not eating close to bedtime
The best practice is to finish your last meal 2-3 hours before bed. This timing makes a big difference. People who eat less than 3 hours before bed face 7.45 times higher odds of GERD compared to those who wait 4+ hours. Acid flows up into your esophagus much easier without gravity’s help when your stomach is full.
Staying upright after meals
Your body needs you to stay upright for at least an hour after eating. Standing or sitting helps gravity keep stomach acid in place. Your esophagus should always stay above your stomach level. Skip intense workouts for a couple hours after meals, though a relaxed evening walk works fine.
Do You Need A Stomach Doctor?
Dr. James Maher, like many gastroenterologists, suggests starting with these natural approaches for most acid reflux patients. When you pay attention to these lifestyle factors, you can take charge of your symptoms instead of letting them run your life. These straightforward but powerful changes could reshape your daily comfort and digestive health for years to come. Reach out to Dr. James Maher.
Acid Reflux FAQs
What are helpful lifestyle changes to manage acid reflux?
Effective lifestyle changes include eating smaller, more frequent meals, avoiding trigger foods like fried items and citrus, incorporating high-fiber foods, not eating close to bedtime, and staying upright after meals. These adjustments can reduce acid reflux symptoms.
Which foods can help alleviate acid reflux symptoms?
Foods that can help alleviate acid reflux symptoms include high-fiber options like oatmeal and root vegetables, alkaline foods such as bananas and melons, and watery foods like cucumber and lettuce. These foods can help neutralize stomach acid and promote better digestion.
How long should I wait after eating before lying down?
It’s recommended to wait at least 2-3 hours after eating before lying down. This allows time for proper digestion and reduces the risk of acid flowing back into the esophagus. Maintaining this interval between dinner and bedtime can significantly lower the odds of experiencing GERD symptoms.
Can chewing gum help with acid reflux?
Yes, chewing gum after meals can help with acid reflux. Studies have shown that chewing gum can reduce acid contact time in the esophagus for up to three hours after a meal. This simple habit can be an effective part of managing acid reflux symptoms.
How does meal size affect acid reflux?
Meal size significantly affects acid reflux. Larger meals can lead to more reflux episodes and longer acid exposure times. Consuming smaller, more frequent meals throughout the day can help maintain steady digestion and reduce the likelihood of experiencing acid reflux symptoms.
Nearly 60 million Americans experience heartburn as a monthly issue that needs attention from a GERD doctor. Regular heartburn affects many, but recurring symptoms might indicate a more serious condition. Your heartburn episodes occurring more than twice weekly could point to Gastroesophageal Reflux Disease (GERD). The condition develops at the time your lower esophageal closure weakens or relaxes the wrong way.
What is the difference between acid reflux, heartburn, and GERD?
Acid reflux, heartburn, and GERD often get mixed up, but each means something different about your digestive health. Learning these differences will help you know if home solutions are enough or if you need to see a GERD doctor.
Acid reflux
Acid reflux happens when your stomach contents flow backward into your esophagus. Your stomach and esophagus have a ring-shaped muscle between them, called the lower esophageal sphincter, that doesn’t close properly after eating. This sphincter works like a one-way valve that can sometimes malfunction.
Many people don’t even notice when they have occasional acid reflux. Others feel uncomfortable after meals, especially if they lie down or bend over. Doctors call this backflow gastroesophageal reflux (GER). Some triggers include eating big meals, specific foods and drinks, bending over after eating, and going to bed after meals.
Heartburn
Your heart isn’t involved in heartburn at all. It’s actually the main symptom of acid reflux. You feel a painful, burning sensation behind your breastbone. This happens because your esophagus doesn’t have the protective mucous lining that your stomach has to guard against stomach acid. You’ll usually feel heartburn within an hour after eating, particularly after a big meal. The pain can spread to your neck, throat, or back and gets worse when you bend, exercise, or lie down. On top of that, it can leave a bitter or sour taste in your mouth.
GERD
Gastroesophageal reflux disease (GERD) is acid reflux in its chronic, more severe form. Medical experts say GERD affects about 20% of adults and 10% of children in the United States. You develop GERD when acid reflux happens regularly over a long time. The biggest difference between simple acid reflux and GERD is how often it happens, how long it lasts, and whether it damages tissue. GERD causes repeated symptoms that bother you or lead to complications over time.
GERD can cause inflammation in your esophagus, which might lead to a few things.
Esophagitis (inflammation of the esophagus)
Esophageal strictures (narrowing)
Barrett’s esophagus (cell changes that might cause cancer)
Dental damage from stomach acid
Chronic cough or asthma-like symptoms
GERD can disrupt your sleep and daily activities if left untreated. Some patients get unusual symptoms like chronic cough, sore throat, or hoarseness that might not seem related to digestion.
Knowing how occasional acid reflux can turn into chronic GERD helps you decide when to get professional help. Dr. James Maher helps diagnose and treat these conditions. He creates customized GERD treatment plans based on how severe your symptoms are and your medical history.
Signs that your heartburn may be GERD
You need to spot the warning signs that show if your heartburn is actually GERD. This knowledge helps you decide when it’s time to see a doctor. Some symptoms need a GERD specialist’s evaluation beyond just dealing with mild discomfort.
Frequent heartburn
Most people get heartburn now and then. However, experiencing heartburn more than twice a week for several weeks points to GERD rather than simple acid reflux. Doctors see this pattern as a strong sign of GERD. You should see a doctor if your heartburn keeps coming back most days despite changes in your habits or using over-the-counter medicines.
Pain or difficulty swallowing
Doctors call it dysphagia when you have trouble swallowing. This problem often shows up after GERD damages your esophagus. Food might feel stuck in your chest, or you might feel pain while swallowing. Your esophagus gets irritated from repeated acid exposure, which leads to inflammation and possible scarring that narrows the passage. These symptoms need attention fast because untreated swallowing problems can lead to dehydration, poor nutrition, or choking risks.
Chronic cough or sore throat
GERD tops the list of chronic cough causes, even in people who don’t notice obvious heartburn. This happens because your vagus nerve triggers protective coughing, or tiny acid drops reach your throat and airways. Watch for coughing that gets worse at night, after eating, or when you lie down. A constantly scratchy throat, hoarse voice, or feeling something stuck in your throat might mean acid is reaching your upper airway.
Regurgitation of food or sour liquid
Stomach contents can back up into your mouth, bringing an acidic or bitter taste. About 70% of people with GERD deal with this problem. The symptoms get worse when you bend over, lie down, or eat. This is not like vomiting since you won’t feel nauseous or have stomach contractions.
Chest pain that mimics heart issues
GERD can cause chest pain that feels like heart problems. Instead of burning, you might feel intense pressure or sharp pain under your skin. GERD pain usually stays the same during exercise, unlike heart-related chest pain. Since telling these apart is tricky, you should get medical help right away for any unexplained chest pain.
When to see a GERD specialist??
It’s not always easy to know the right time to see a gastroenterologist about digestive symptoms. Dr. James Maher, a gastroenterology specialist with decades of experience, shares several specific situations that warrant professional evaluation.
Symptoms not improving with OTC meds
Your symptoms might need a professional gastroenterologist’s evaluation if self-treatment with over-the-counter medications isn’t working. Proton pump inhibitors (PPIs) help patients with just one daily dose. You should schedule an appointment if these things are happening!
Your heartburn medication hasn’t helped after two weeks
Need over-the-counter medications more than twice weekly
Taking medication at the right time (30-45 minutes before meals) hasn’t worked
Dr. Maher will determine if you need prescription-strength medication or if your symptoms point to something other than GERD.
Heartburn disrupting daily life or sleep
GERD can affect your quality of life by a lot when symptoms get in the way of daily activities. Research shows that patients with heartburn-predominant symptoms face sleep interruptions, eating or drinking problems, and work disruptions. Dr. Maher knows that good sleep is vital, so he might suggest raising your bed’s head among other targeted treatments.
Unexplained weight loss or vomiting
Some symptoms need immediate medical attention because they could indicate serious complications. You should contact gastroenterologist Dr. Maher right away if you experience unexplained weight loss, poor appetite, ongoing vomiting, or food coming back up. These signs could mean esophageal damage or other digestive problems that need specialized evaluation. Untreated GERD might lead to Barrett’s esophagus, which raises your risk of esophageal cancer.
Family history of esophageal issues
Your genes can affect your GERD risk by a lot. Studies show that people whose immediate family members have heartburn or esophageal disease are more likely to have reflux symptoms. Dr. Maher takes special care to get a full picture of your family history to create customized treatment plans. If your relatives have had Barrett’s esophagus, esophageal strictures, or digestive tract cancers, you might benefit from earlier and more frequent screenings.
Do You Need Stomach Help?
Dr. James Maher’s gastroenterology expertise lies in diagnosing and treating these conditions. He provides customized care based on each patient’s symptoms and medical history. His background as a gastroenterology specialist helps create complete treatment plans that fit your specific situation. Getting help early can prevent bigger problems down the road. These warning signs are worth your attention, and reaching out to a qualified GERD specialist like Dr. Maher could be your first step toward lasting relief and better health.
GERD FAQs
When should I consult a doctor about my heartburn?
You should consult a doctor if you experience heartburn more than twice a week, if over-the-counter medications don’t provide relief, or if your symptoms are interfering with your daily life or sleep. Additionally, seek medical attention if you have difficulty swallowing, unexplained weight loss, or persistent vomiting.
What are the warning signs that my heartburn might be GERD?
Warning signs include frequent heartburn (more than twice a week), pain or difficulty swallowing, chronic cough or sore throat, regurgitation of food or sour liquid, and chest pain that mimics heart issues. If you experience these symptoms persistently, it’s important to consult a gastroenterology specialist.
How can I differentiate between occasional heartburn and GERD?
Occasional heartburn is typically infrequent and can be managed with lifestyle changes or over-the-counter medications. GERD, on the other hand, involves chronic acid reflux occurring twice weekly or more, often causing persistent symptoms and potential complications like esophageal inflammation or strictures.
Are there any serious complications associated with untreated GERD?
Yes, untreated GERD can lead to serious complications such as esophagitis (inflammation of the esophagus), esophageal strictures (narrowing), Barrett’s esophagus (cell changes that may lead to cancer), dental erosion, and chronic respiratory issues like persistent cough or asthma-like symptoms.
Does family history play a role in GERD risk?
Yes, genetics can influence your risk of developing GERD. If you have immediate family members with heartburn or esophageal issues, you may be more likely to experience reflux symptoms. In such cases, earlier and more frequent screenings may be beneficial, especially if relatives have had conditions like Barrett’s esophagus or esophageal cancer.
A high-fiber diet can provide many health benefits. Firstly, it may help treat chronic constipation and improve the quality of stool. Moreover, a high-fiber diet may also decrease the incidence of colon cancer while also improving markers of fecal inflammation and intestinal symbiosis in parties with Inflammatory Bowel Disease.
Struggling with constipation? Try a high-fiber diet and contact Katy Stomach Doctor!
A consultation with a gastroenterologist will provide more insight into the benefits of a high-fiber diet, specifically how it can benefit you. A study recently compared Kiwi fruit, prunes, and psyllium for the treatment of chronic constipation. The study found that consuming kiwi results in less bloating. Moreover, kiwi offers the greatest improvement in stool quality in comparison to the other options.
Dr. James Maher is here to help you achieve a healthy gut.
If you have recently started struggling with constipation then a consultation with a gastroenterologist would be best. A consultation allows for further evaluation of possible causes including colon cancer and other obstructive lessons. In the absence of any findings, a high-fiber diet is usually recommended. Most dietary fiber and fiber supplements result in gas and bloating. According to the previously mentioned study, kiwi appears to be more tolerable. If you’d like to schedule a consultation with an experienced and trusted gastroenterologist, contact Katy Stomach Doctor today.
There are multiple treatment options available for managing obesity. This is due to an estimate of 60% of the US population suffering from some degree of obesity. Before exploring options, a baseline assessment of nutritional and medical status should be complete. There is an increased risk of diabetes, hypertension, and cardiovascular disease in patients who suffer from obesity. Other risk factors include an increased risk of liver cancer, colon cancer, and pancreatic cancer.
Before you explore treatment options, you should receive an evaluation by a gastroenterologist. NAFLD (fatty liver) is now the most common cause of end-stage liver disease in the U.S. This disease occurs in the pediatric age group as well as young adults. Since the findings on laboratory evaluations and physical examination are often very subtle. Again, a consultation with a gastroenterologist would be helpful.
A balanced diet is the first step to overcoming obesity.
Treatment Options & Food Plans
Specific options for the treatment of weight loss include the following: lifestyle modifications, medications, and bariatric surgery. The cornerstone of any treatment regimen is caloric restriction and exercise. Calorie restriction of 1200-15000 calories per day is essential to managing your weight. Most patients who do not lose weight with intake restrictions are underestimating calorie intake.
Food plans are a highly effective method for maintaining and improving weight loss. To ensure your food plan is as effective a possible, you should weigh and measure your food intake. Four ounces of chicken after cooking is about 2 good bites. Although multiple different diets have been promoted, no one diet has been found to be superior. There are no studies that suggest the keto diet is better than the Mediterranean and vice versa.
Whatever diet you chose, it has to be palatable. Since calorie restriction is indefinite, the diet also has to be something reasonably sustainable. In addition to calorie restriction, weekly physical exercise is essential. 150 hours a week of aerobic exercise plus resistance training is just one of many options for physical exercise. It should be noted that exercise alone will not result in significant weight loss. However, it will help maintain weight loss.
Consult with Dr. James Maher today!
Managing Obesity with Medication
Several different medications have been FDA approved for weight loss. This includes phentermine, orlistat, naltrexone/bupropion, and liraglutide. The choice of drug therapy is a balance between efficacy, adverse effects, and patients’ other medical problems. Consulting with a nutritionist and gastroenterologist will help determine the best option for you. If 5% or more weight loss doesn’t occur within three months, you should discontinue your medication.
The last option is bariatric surgery. Gastric balloons have become increasingly popular and offer varying success. Gastric balloons can result in obstruction, gastric ulcerations, and abdominal pain. Endoscopic remodeling results in a type of restrictive surgery with varying degrees of success.
With that in mind, bariatric surgery is an option strictly for patients with a BMI greater than 40 or over 35 with medical problems associated with obesity. Two operations are commonly available; the gastric sleeve and the Roux-en-y. The gastric sleeve removes a portion of the stomach, while the Roux-en-y gastric bypass is more invasive with a 12% complication rate. Although there is a higher complication rate, it results in a significantly higher weight loss.
Obesity is a national epidemic affecting all age groups and genders. Aggressive lifestyle medication associated with calorie restriction is the basis of any program. An aggressive approach with a consultation should be considered. Consult with Dr. James Maher today to learn the best option for you.
In an observational study, the use of Famotidine (Pepcid) was associated with a lower incidence of mortality, a lower chance of intubation, and lower inflammatory markers. The reason for this association is unclear. Famotidine inhibits histamine release which is found in most tissue. The release of histamine causes a cascade of other inflammatory cytokines and proteases to be release.
Call today to consult with a professional gastroenterologist.
Viruses, including COVID, act on cells in the lung to cause histamine release. It is postulated that blocking histamine release, reduces the inflammatory response to this viral infection. It appears that PPIs (Proton pump inhibitors) have the opposite effect. By taking PPIs, you can increase the risk of COVID positivity. However, the increased risk is dose dependant.
You should take the medication once a day as two daily doses could increase the chance of COVID positivity. The PPIs decrease stomach acid secretion. Stomach acid plants an important role in destroying ingested bacteria and viruses. Without gastric acid, patients are at an increased risk for enteric infections including COVID 19. The GI tract is a major conduit for COVID infections invading the small bowel cells which can result in the inflammation of the stomach, small bowel, and colon.
Dr. James Maher is board-certified in both Internal Medicine and Gastroenterology.
PPIs are immensely popular drugs. It seems that everyone takes these medications. However, the medications usually don’t require chronic use. Most GI conditions require three months of treatment then taper off. Due to the rebound hyperacidity, the longer the drug is taken, the more difficult it is to stop. Consultation with a GI specialist will assist in determining the appropriate use of these medications.
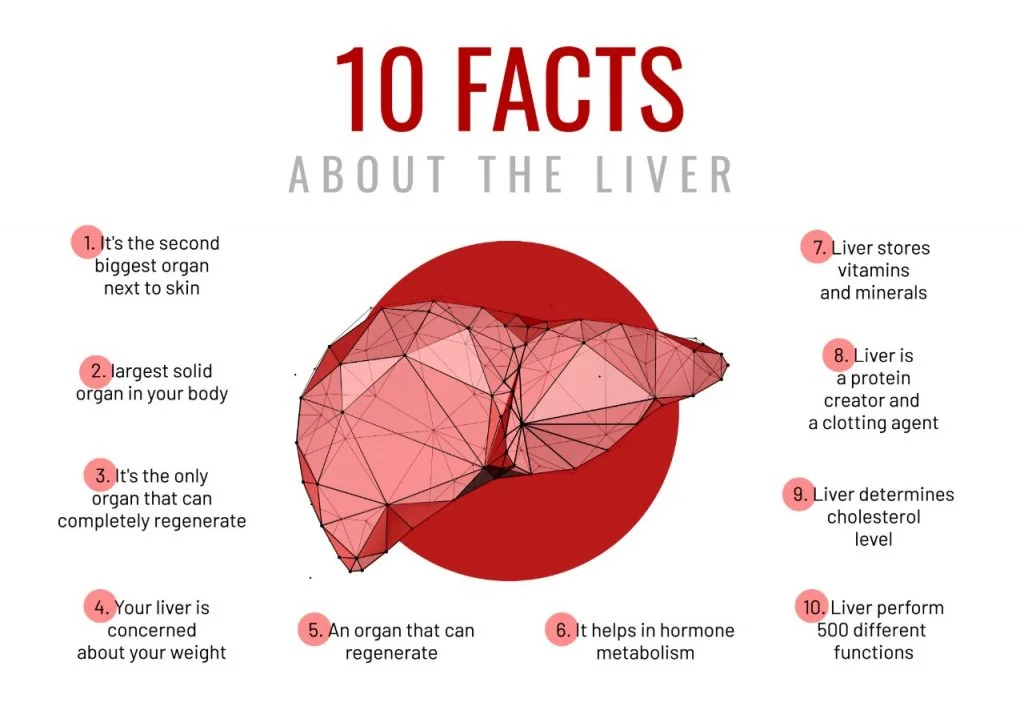
Non-alcoholic liver disease (NALD) refers to a range of liver conditions that affect people who consume little to no alcohol. It is characterized by an increase in fat accumulation in the liver without a significant alcohol presence. NALD is associated with Type 2 diabetes, hypertension, and hyperlipidemia.
This disease is present in at least 80% of patients who have a BMI of more than 35. Additionally, it is more common in women who have a waist circumference over 80 cm and in men whose waist circumference is more than 102 cm. Insulin resistance is the central feature of metabolic syndrome.
Learn of your likelihood of catching NALD by speaking with our professional team.
Macrophages in fat produce inflammatory enzymes that break down fat in tissue used predominantly by muscle and other tissue. This inhibits sugar utilization resulting in hyperglycemia, leading to elevated insulin levels. As a result, fatty acid production in the body will further increase.
The over-production of fatty acids leads to elevated triglyceride levels with increased liver fat. This will progressively lead to increased fat in the liver and the development of fibrosis and NASH.
Fibrosis can lead to worsening liver disease and eventually cirrhosis. Nonalcoholic fatty liver disease (NAFLD) is the most common cause of liver disease in this country. The disease is very common in children 12-18 years old and can also affect young adults and pregnant women.
If you’d like more information regarding Nonalcoholic Liver Disease, contact Dr. James Maher today!
Studies & Screening Options
In a recent study, the disease was progressive in 23% of children, even those with dietary therapy. Obesity and elevated liver enzymes alone underestimate the presence of NAFLD. A liver biopsy is accurate but invasive. A Fibro scan, which measures liver stiffness, has limitations but is currently used for screening.
In the presence of obesity, elevated liver enzymes, or upper abdominal pain, a consultation with a gastroenterologist familiar with this disease is recommended. Multiple drug research trials are currently in progress. If qualified, a referral for a drug trial can easily be done if a patient qualifies. A gastroenterologist can monitor for disease progression and the development of liver cancer.
Colorectal Cancer is the second most common cancer. If diagnosed earlier, the cancer is curable with colonoscopy or surgical resection. However, once the tumor has spread to regional lymph nodes, liver or lung life expectancy is reduced.
Several options are available for colon cancer screening. The stool testing for guaiac has largely been replaced by fecal immunochemical tests. This offers a reasonably accurate and inexpensive screening test for colorectal cancer and advanced cancer. However, it may not be so accurate at detecting large polyps and early cancer.
Another stool testing option includes multitargeted stool DNA (Cologuard). This stool test is relatively new and is more sensitive than the FIT stool test. Additionally, the Cologuard stool exam is more expensive than the FIT exam.
Of course, Colonoscopy remains the most accurate screening test, and the only examination which can remove precancerous polyps and early cancer. With a normal colonoscopy in an average risk patient, repeat colonoscopy is not recommended for 10 years, and the risk of developing colon cancer is greatly diminished for 17 years.
If the patient is at risk risk for developing colon cancer, then colonoscopy is the preferred examination. Otherwise any option, including stool tests or colonoscopy, is acceptable. If the stool test is positive, then proceeding with a colonoscopy is necessary.
The Stool test requires repeating at frequent intervals whereas the colonoscopy is more sensitive and usually requires less frequent examinations. Most importantly, any of the above examinations are better than doing nothing. Consultation with a GI specialist who performs colonoscopies will help determine the best choice.
Daily Aspirin intake reduces the risk of colorectal cancer in high-risk Lynch Syndrome carriers. Lynch Syndrome is the most common hereditary cause of colon cancer; accounting for 5% of colorectal cancer.
In observational trials, daily Aspirin intake has been show to decrease Colorectal Cancer in average risk patients by 20-40%. These potential benefits of long-term therapy must be weighed against potential adverse effects including gastrointestinal bleeding and renal toxicity.
Consulting with a GI specialist will help determine whether this preventive therapy is advisable.
With effective treatment of Hepatitis C and Hepatitis B, fatty liver is now the most common cause of liver disease in the US. Although it has no clear cause, fatty liver is linked to obesity, insulin resistance, hypertension, heart disease, and elevated cholesterol. Certain ethnic groups, especially Hispanics, have a higher prevalence of fatty liver.
Most commonly, fatty liver does not cause any specific symptoms. However, it may cause mild fatigue and dull right upper abdominal pain. This is due to the stretching of Gleason’s capsule. It can also cause a mild elevation of liver enzymes.
Since no specific blood tests are available to diagnose fatty liver, other types of liver disease will need to be ruled out. This includes testing for alcohol intake, as well as blood tests to rule out Hep B, Hep C, and Wilson’s Disease. Medication history in the patient will help rule out drug reaction.
Usually, fatty liver is diagnosed by an imaging study. On abdominal ultrasound, the liver has increased echo patterns suggestive of increased hepatic density. More specific tests include a FibroScan, which measures liver density. Although not always necessary, liver biopsy can confirm the diagnosis and severity of the liver disease.
Fatty liver itself does not cause any significant liver dysfunction. It does, however, indicate significant metabolic problems, including an increased risk of developing diabetes, hypertension, and heart disease. However, fatty liver can progress into nonalcoholic steatohepatitis (NASH).
On liver biopsy, NASH looks just like an alcoholic liver disease with increased fat and fibrosis. If this occurs, consultation with a GI specialist is recommended. NASH can progress to cirrhosis, which is end-stage liver disease. Even without progression to cirrhosis, the development of liver cancer (HCC) is increased. Even with the high prevalence of fatty liver, the development of HHC will substantially increase in this country.
Although the treatment of fatty liver is an intense research area, no drug therapy is currently available. Obeticholic acid (OCA) is in phase three trials and shows promise. It has significant side effects such as pruritis and elevation of cholesterol, which may limit its use. If the patient is obese, a limited weight loss of 10% body weight can reverse fibrosis. Although no clinical trial has been published, low-dose aspirin may be of benefit as it can decrease the development of liver cancer.
Fatty liver is now the most common cause of liver disease in this country. Consultation with a GI specialist or liver specialist is recommended for further evaluation and treatment options.
Colorectal Cancer (CRC) is a common and lethal disease. It is estimated that 100,000 cases of CRC are diagnosed in the US annually. Approximately 53,000 Americans are expected to die of CRC every year. Although the mortality rate of CRC is decreasing, it remains the third most common cause of cancer-related death in women and the second most common in men.
Although the incidence of CRC in patients over 50 has been decreasing, CRC incidence in patients aged 40-50 has been increasing. The US Preventative Services Task Force recommends screening for average-risk African Americans at age 45.
The type of screening should be a shared decision between the patient and the GI specialist. Colonoscopy, which is recommended by most GI MD’s is the only screening test proven to decrease CRC mortality. Optimally, this procedure should be performed at 50 in average-risk patients, and if negative, repeated every ten years.
Fecal Immunochemical Testing (FIT) is a stool test done annually and is recommended in patients unable or unwilling to have a colonoscopy. If the FIT result is positive, a colonoscopy must be performed by a GI specialist. FIT is comparable to colonoscopy in the detection of CRC but has a lower detection rate for advanced adenomas, which may harbor localized cancer.
Computed Tomography Colonography (CTC) is an option for patients at risk of complications from sedation or the procedure itself. CTC requires a colonoscopy laxative preparation and is done without sedation. It is relatively sensitive in identifying large polyps, which, if seen, would require a colonoscopy.
Stool for guaiac fecal occult blood is insensitive and requires multiple stool samples. This test has been largely replaced by more specific stool tests (FIT). Most importantly, any option is better than nothing. Many patients believe that without abdominal pain, change in bowel habits, or rectal bleeding, the risk of developing colon cancer is very low. Most patients found to have colon cancer are asymptomatic and average risk. Discussion with a GI specialist will help determine the best option.
Chronic Ulcerative Colitis (CUC) is an inflammatory disease involving the distal colon, although it may extend to involve the entire colon. CUC is characterized by diarrhea commonly associated with rectal bleeding and colicky abdominal pain. Urgency is severe and involves the entire colon; colonic dilation may occur, resulting in perforation. Any type of bloody diarrhea requires consultation with a GI specialist.
Extraintestinal manifestations (infections that occur outside of the intestine) of CUC are common. These include arthritis involving the large joints and ocular problems resulting in blurred vision.
Evaluation of possible ulcerative colitis includes laboratory and radiologic imaging. However, the diagnosis will eventually require colonoscopy done by a GI MD who performs colonoscopies. An endoscopy will evaluate the severity and extent of the inflammation. Colon biopsies will be obtained to establish the diagnosis and exclude other causes of colon inflammation.
In the past, treatments of ulcerative colitis were limited to oral mesalamine and corticosteroids. Although treatment of mild CUC often begins with mesalamine, treatment failures are common. Corticosteroids are often used to treat moderate to severe CUC, but again, treatment failures are common, as are side effects.
Even if clinical response occurs, this regimen cannot be used to maintain remission. Fortunately, multiple biologic therapies are now available with new innovative drugs on the horizon. The current goal of treatment is mucosal healing.
If this can be achieved, then complications of this disease, such as an increased risk of colon cancer, can be avoided. A total colectomy due to perforation or toxic megacolon can also be avoided. This therapy requires monitoring by GI specialists.